
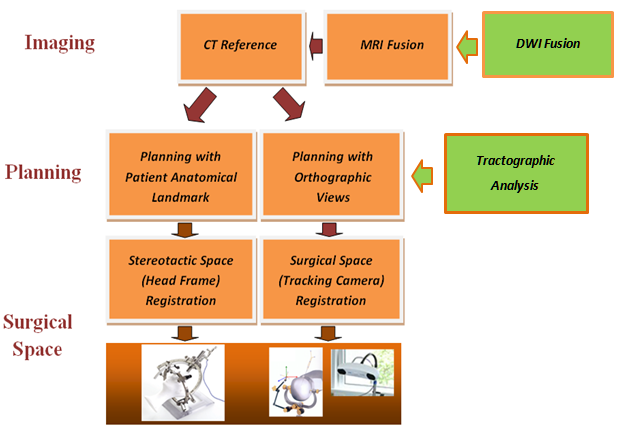
Vister3D is a new prototype of neurosurgical planning platforms for frame-based and frameless stereotactic interventions. Both interventions share the same diagnostic data, - and after archiving, the planning results can be involved in surgical preparation for a different technique. Vister3D offers an ease-of-use planning platform with a generalized solution for conventional arc-based stereotactic head frames:
- •
- •
- •
•
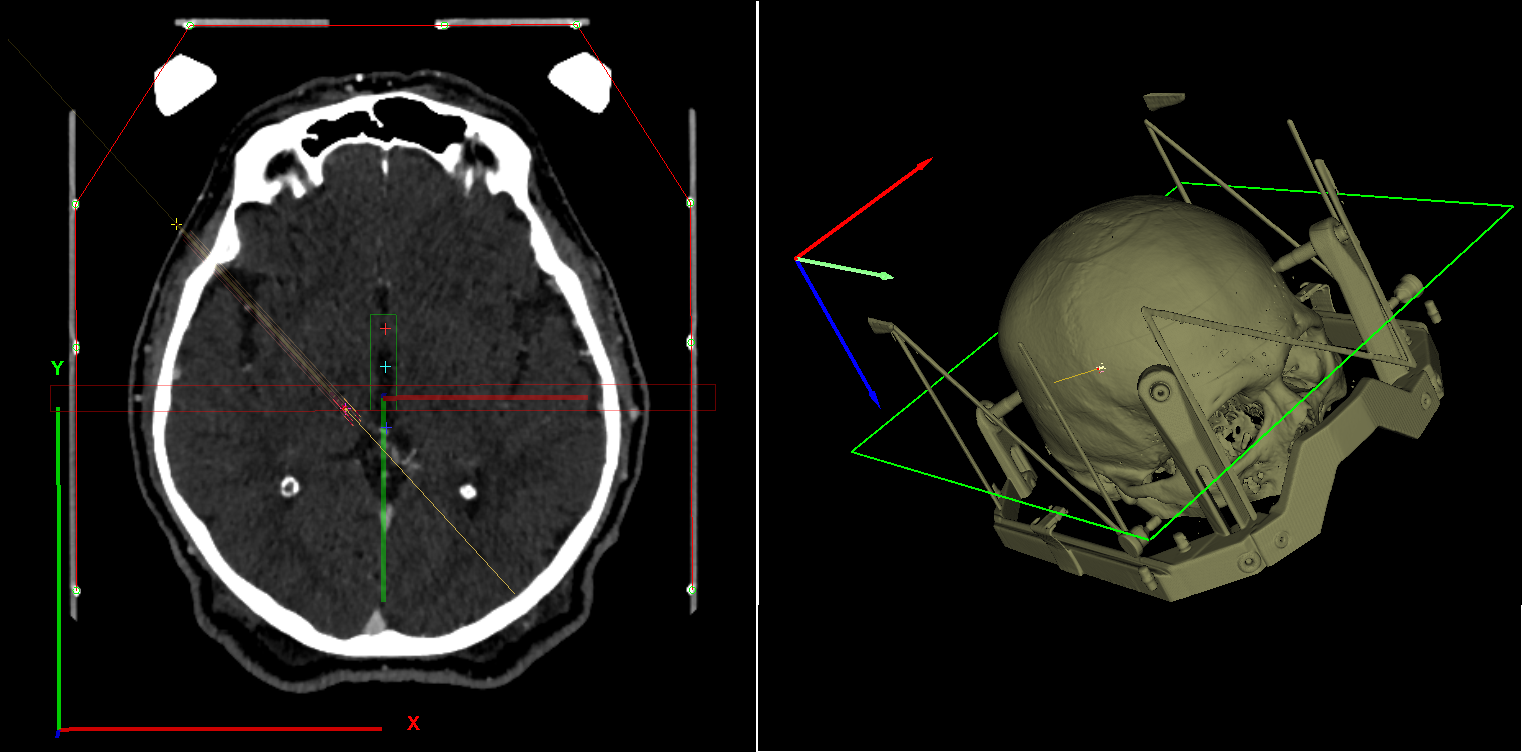
Moreover, the 3D transparency, provided by the software, facilitates accuracy comparisons of frame-based and frameless methods even during the same surgical intervention.
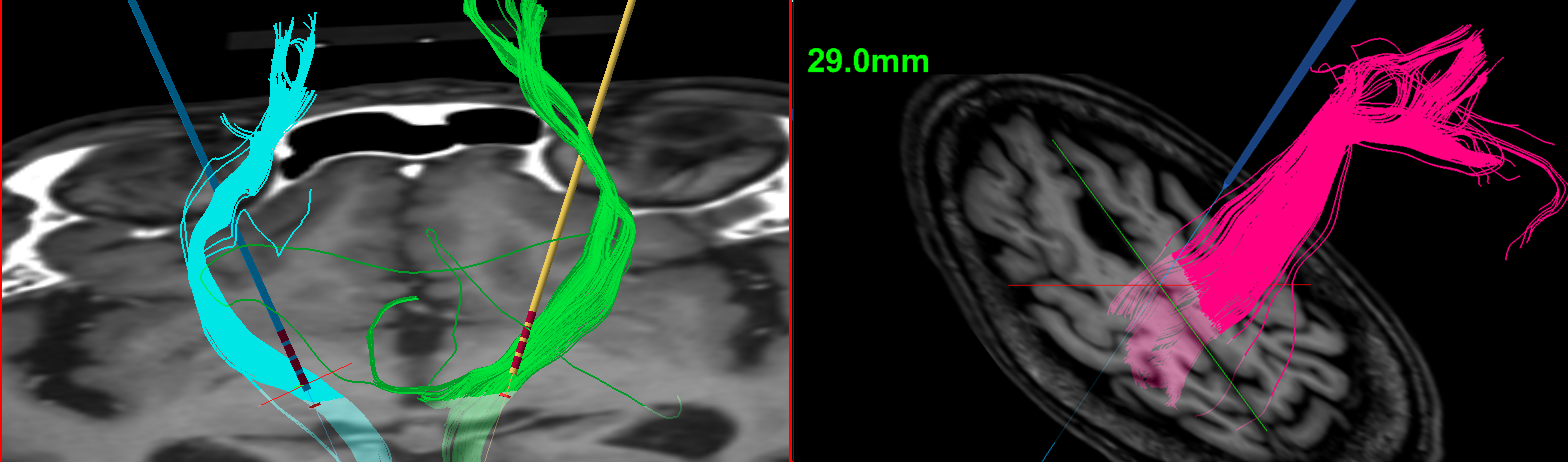
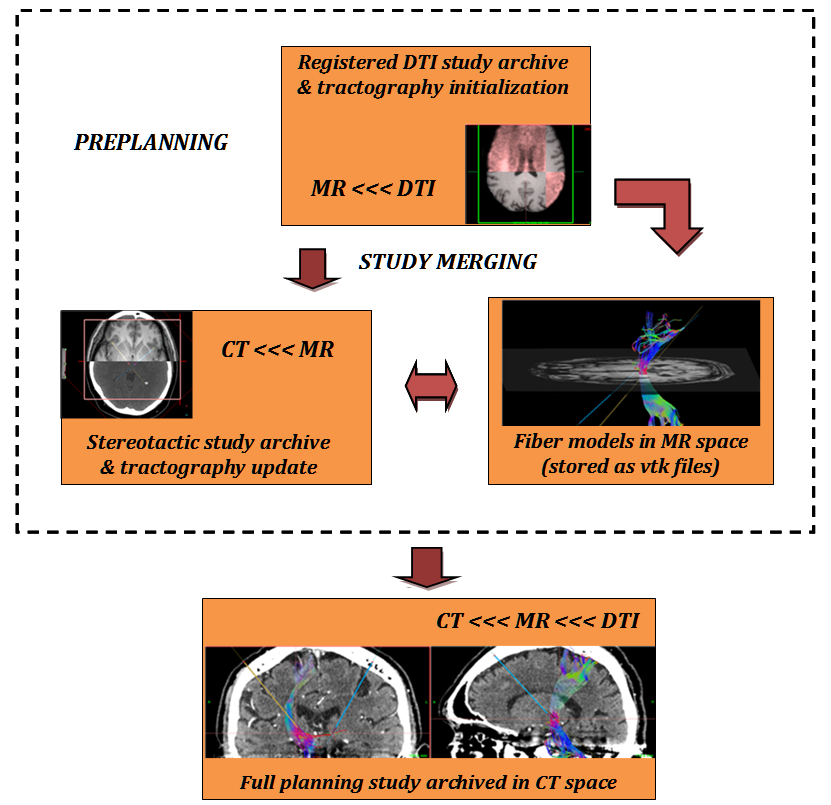
Preplanning is supplemented by DWI (diffusion weighted image) read in and DTI (diffusion tensor imaging) data visualization with GPU-hosted registration to patient MRI. Tractographic analysis can be performed with on-site merging of preregistered archive of fusioned MR and DTI data.
The system has been validated in different brain surgeries:
DBS electrode implantology for Parkinson's disease, tumor biopsy or thermolaesio planning for head-arc, frame-based reference and craniotomy planning for frameless navigation to enhance ablating poorly accessible tumors. The modular architecture supports new feature extensions with immediate use in both methodologies. The complex tasks of adding DTI images and running fiber tractography is enhanced by optional backup of studies in compressed archive at different stages of planning. Knowhow for frame-based stereotaxy is co-owned by qualified neurosurgeon (Dr. István Valálik Ph.D. https://parkinson.hu/) who acts as advisor for software development.
• Patient data module for parsing DICOM data and archive studies from easily maintainable database to improve communication regarding diagnostics. Vister3D planning usually relies on three inputs:
- reference CT (always needed);
- fusion MR (to be registered with reference);
- diffusion tensor imaging (DTI) data (optional for tractography, to be registered with fusion MR);
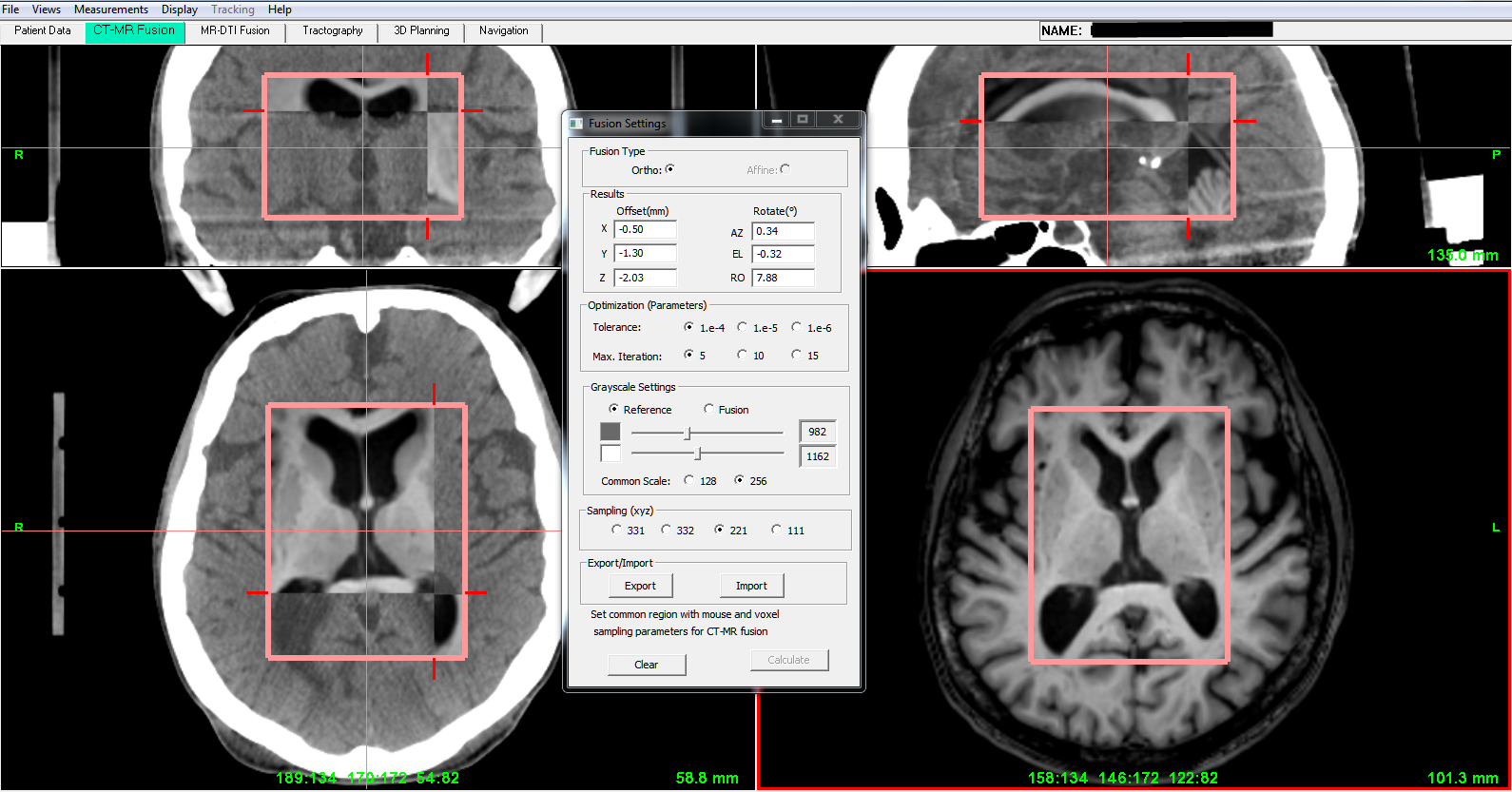
• CT-MR fusion module, targeting user selected subvolume with highly optimized fusion algorithm, aligns MR images to CT and visualizes results in orthographic planes;
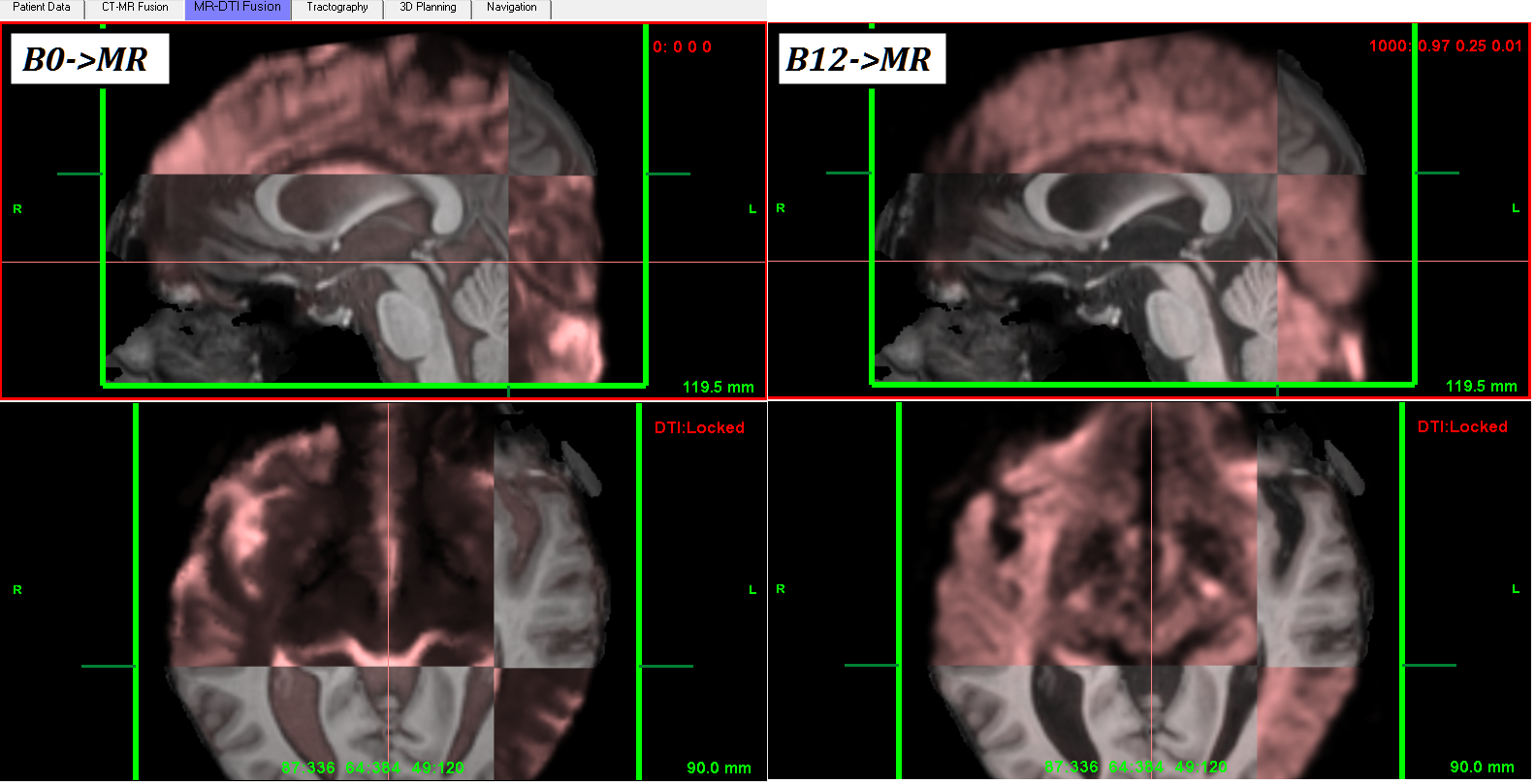
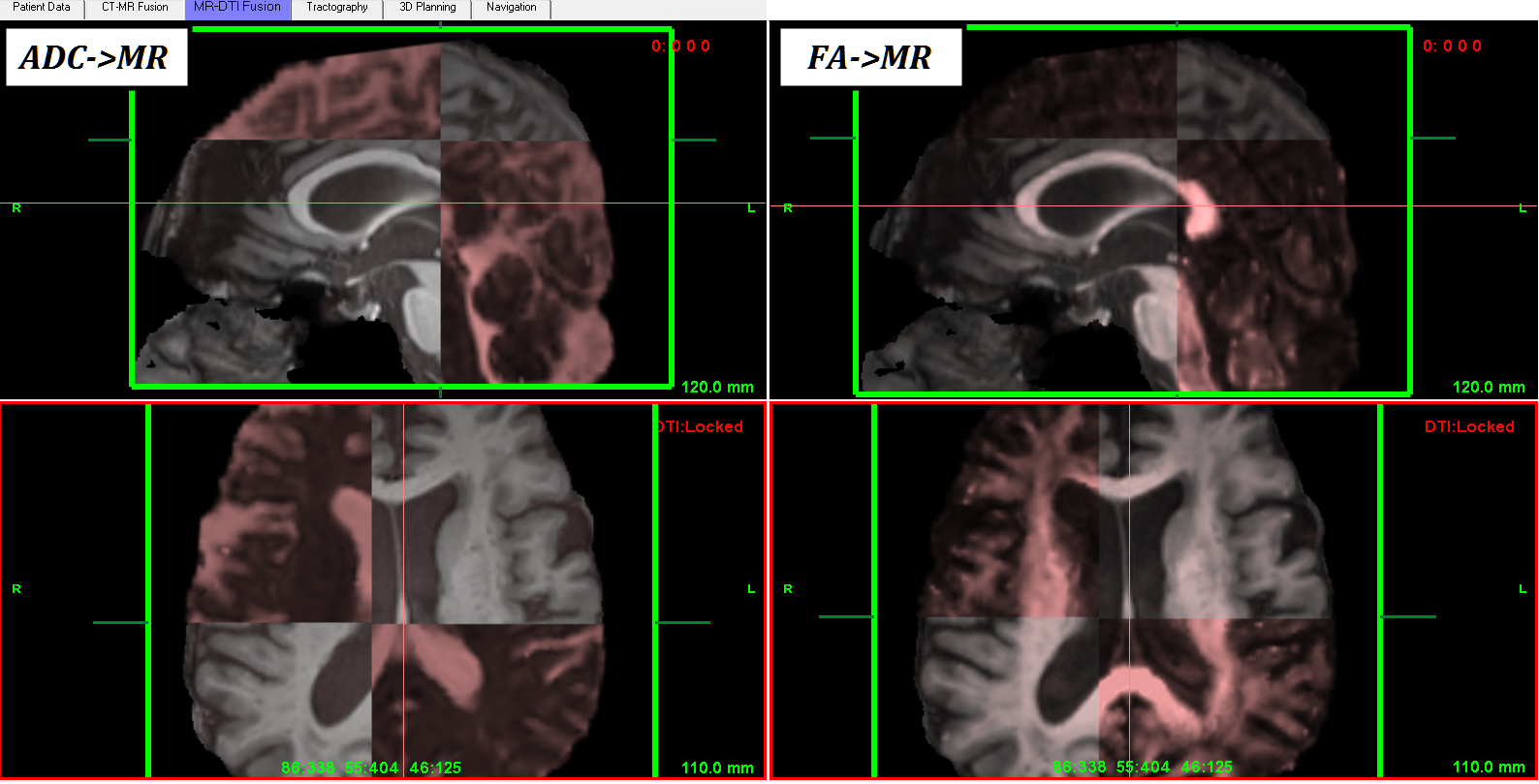
• MR-DTI fusion module, register DWI gradient-weighted dataset to MR (using 0 b-value DTI map, as reference) with fast, CUDA-based algorithm. ADC (mean apparent diffusion coefficient) or FA (fractional anisotropy) maps can be fusioned/displayed with MR for diagnostic purposes;
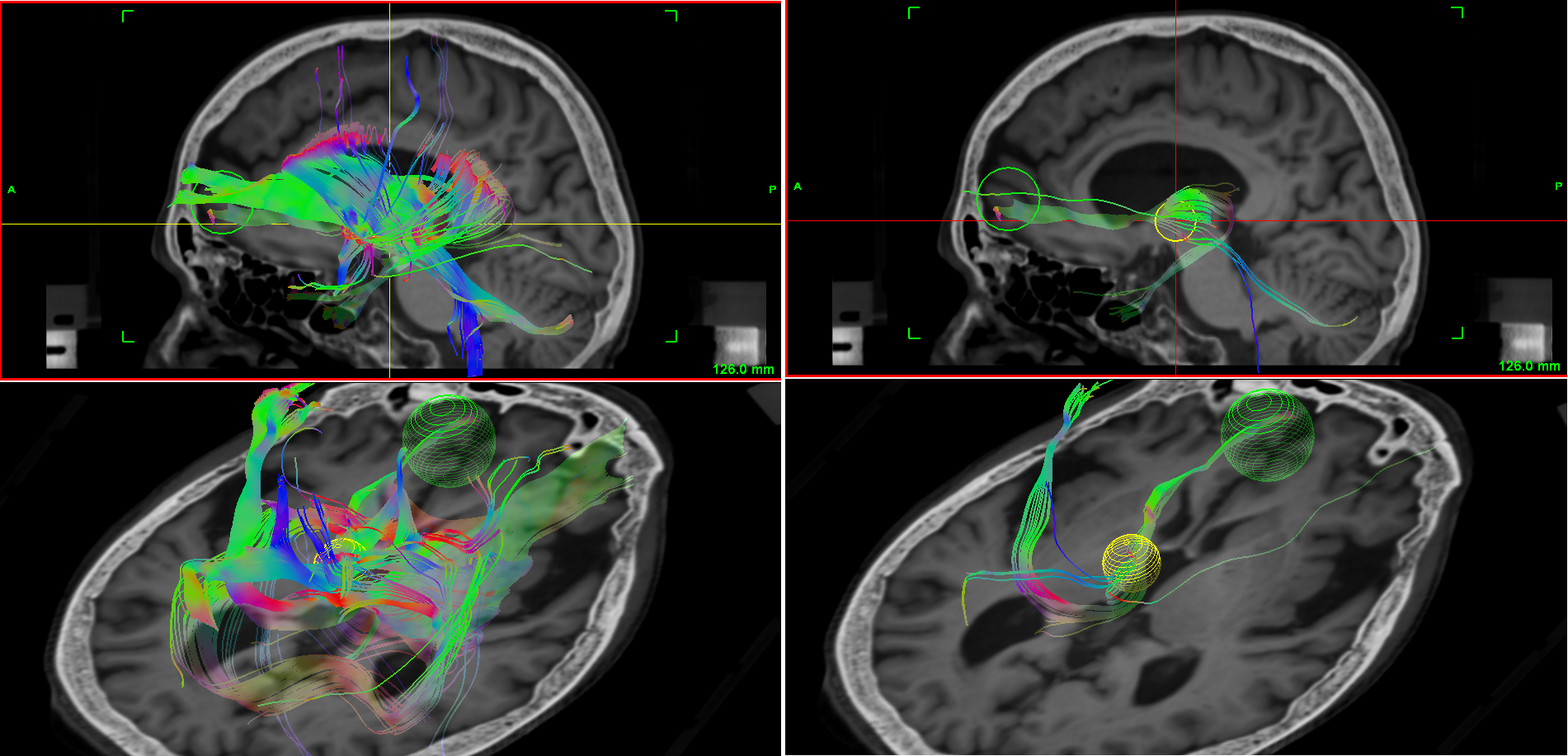
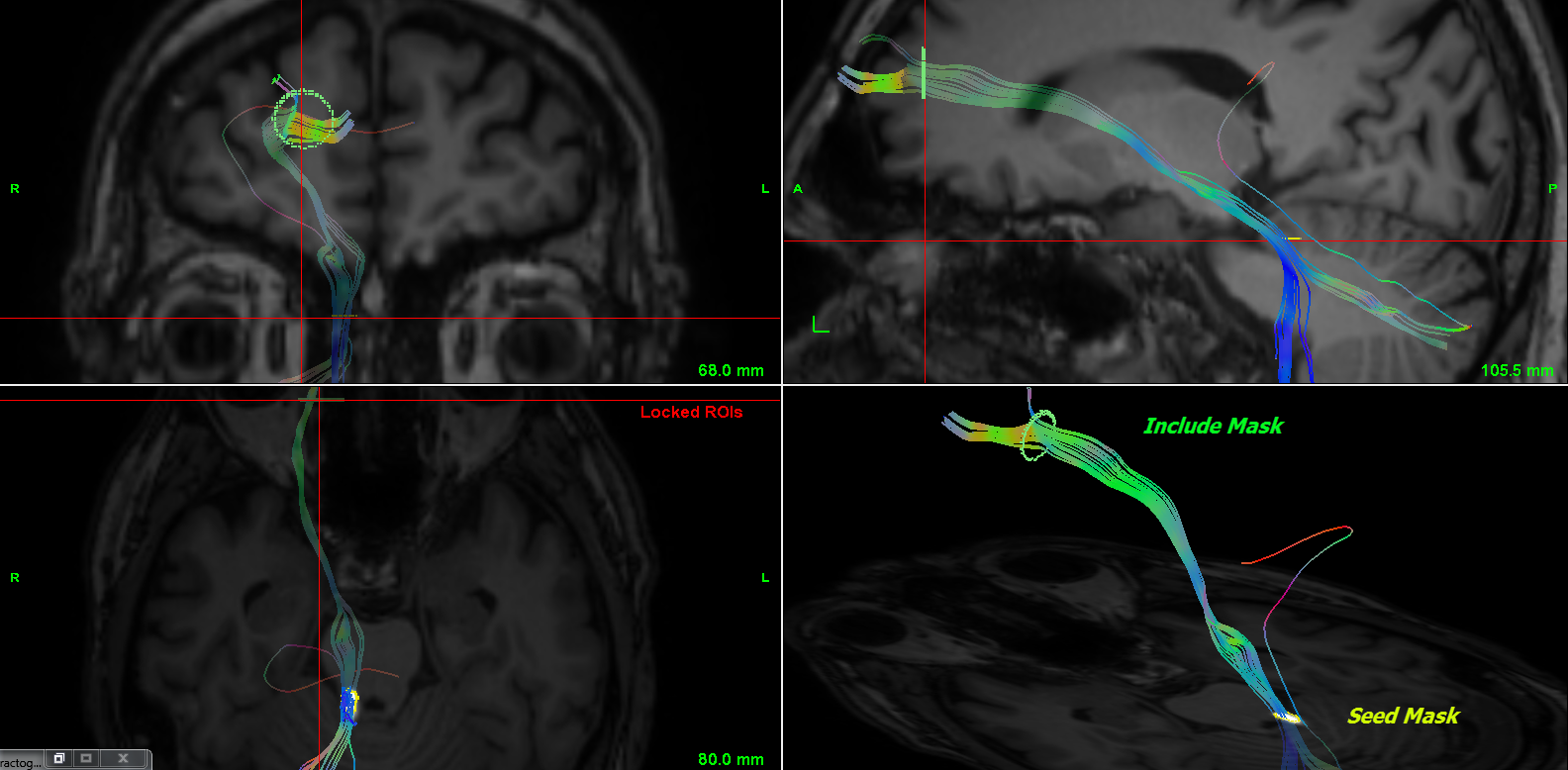
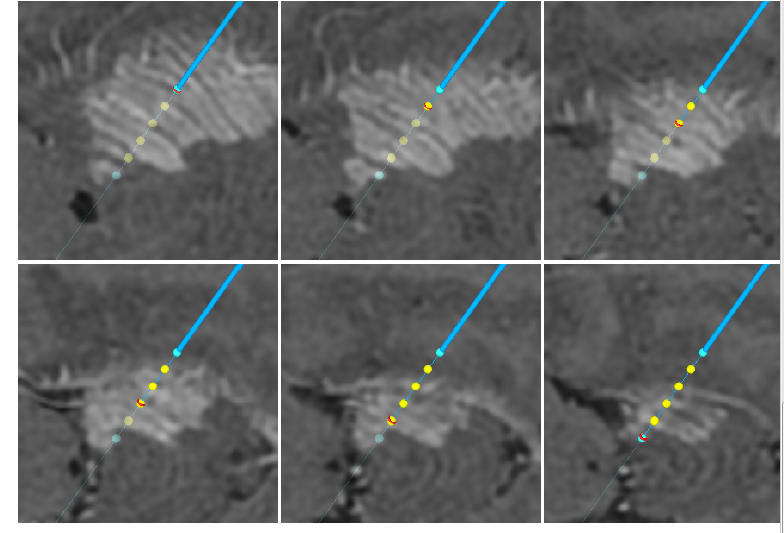
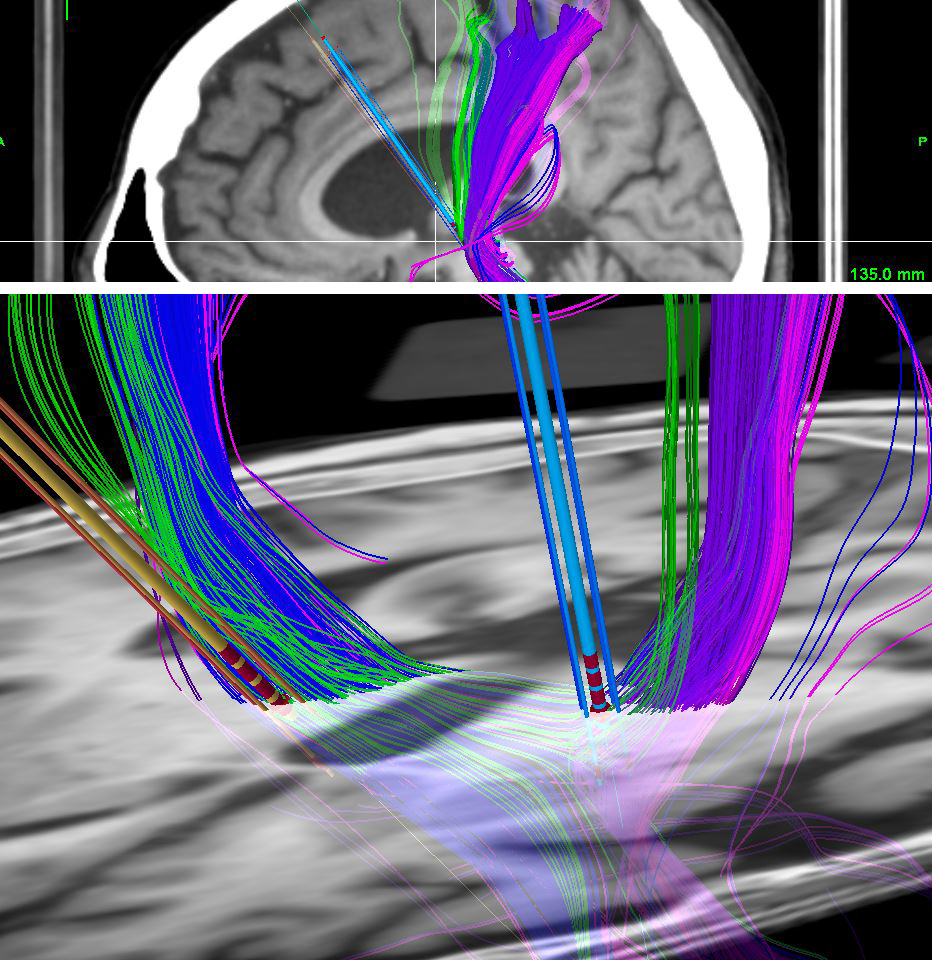
• Tractography module, as planning supplement with automatic parsing of registered DTI data and ROIs positioned on anatomical images. Vister3D implements tractography both on original "raw" data and registered DTI data, as well. The unregistered approach relies on "one session" diagnostics with accurate scanner transform both for anatomical and DTI images;
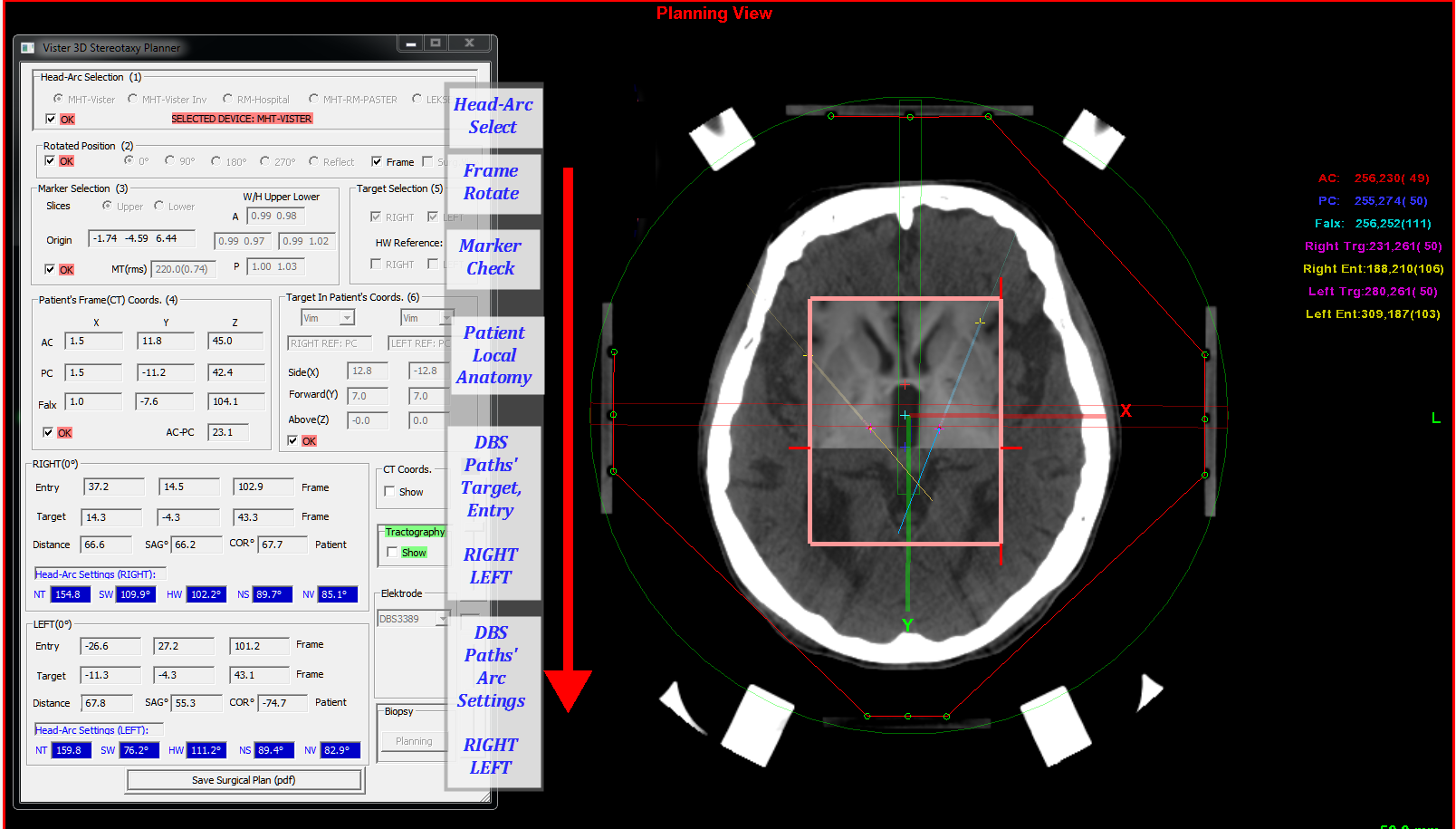
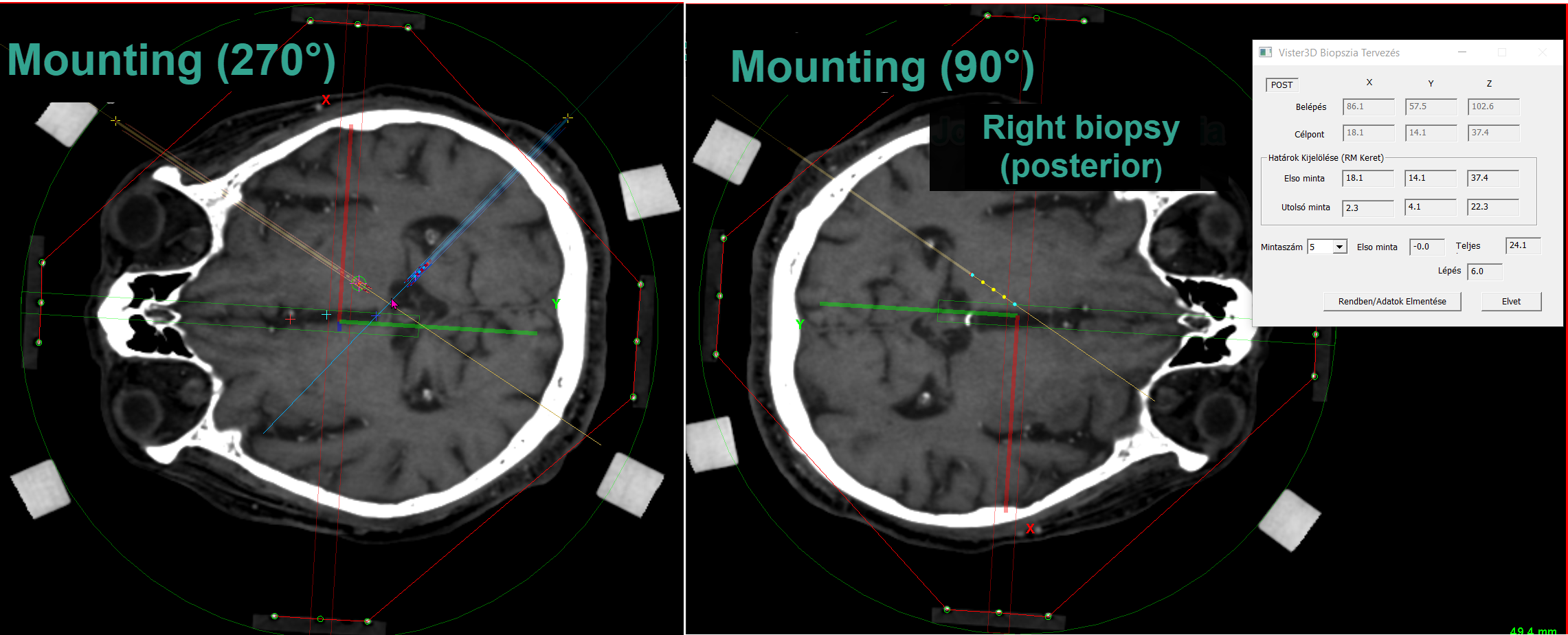
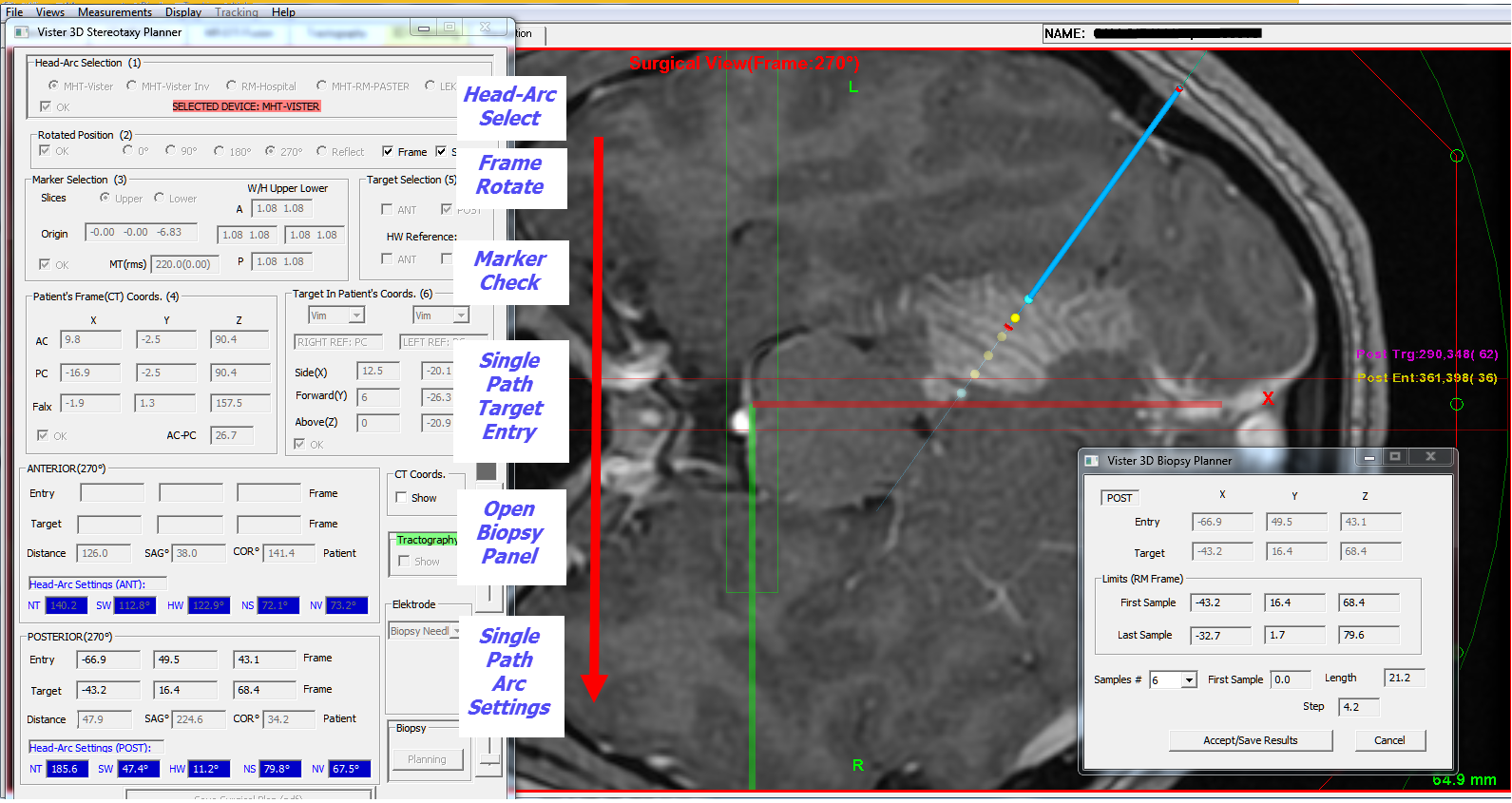
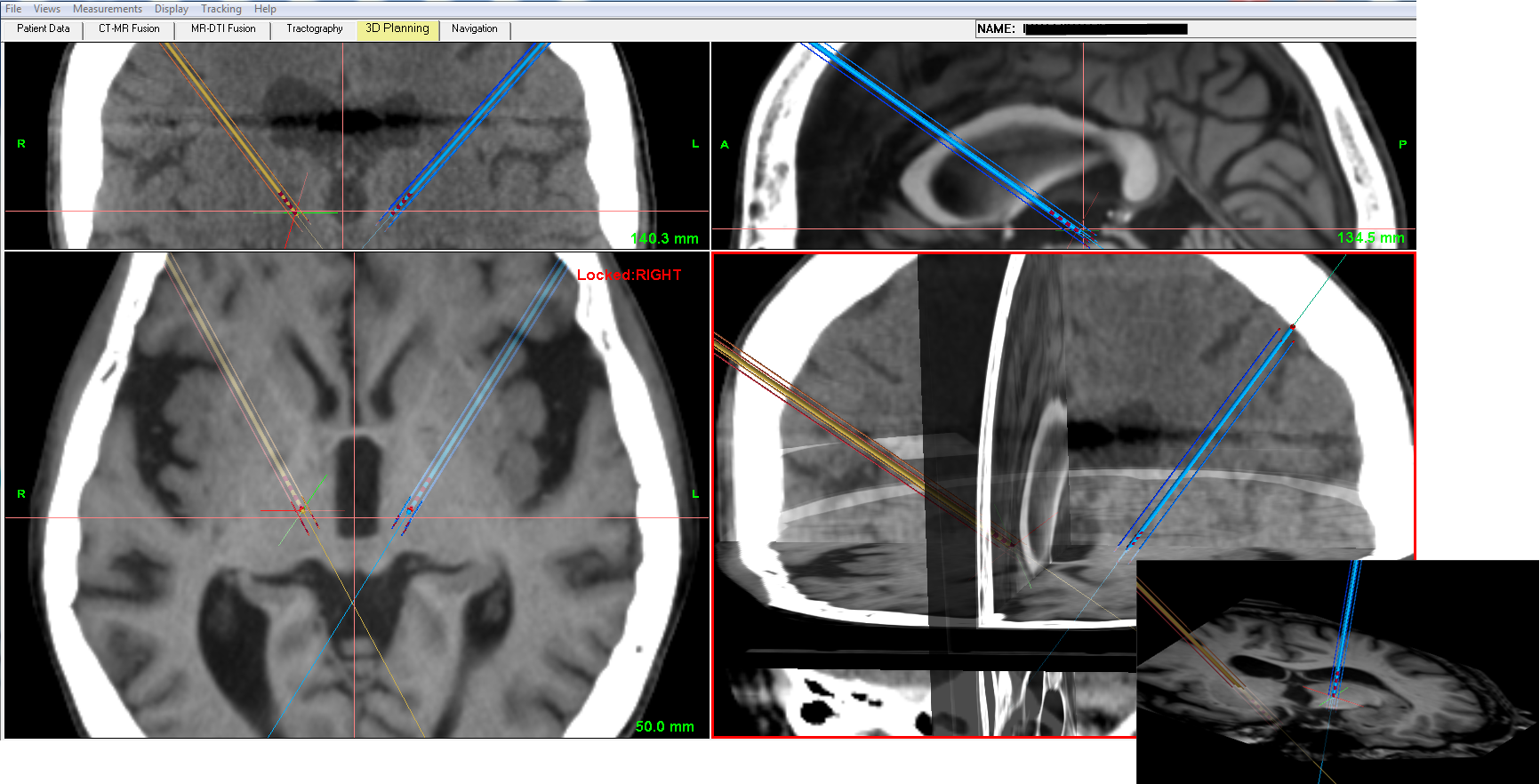
• Planning module integrates all operations needed for frame-based or frameless stereotaxy. The calculations are strictly 3D-based that permits an exchange of planning outcome between different platforms. Some of frame-based systems are supported with calculations optimized for anatomical symmetry. Rotated mounting of frame is also possible using common marker set (Vister3D separates marker- and stereotactic spaces for generalized stereotaxy). Real-time feedback is implemented for displaying errors in marker localization and during trajectory planning for coordinates in image volumes and anatomical spaces along with polar settings;
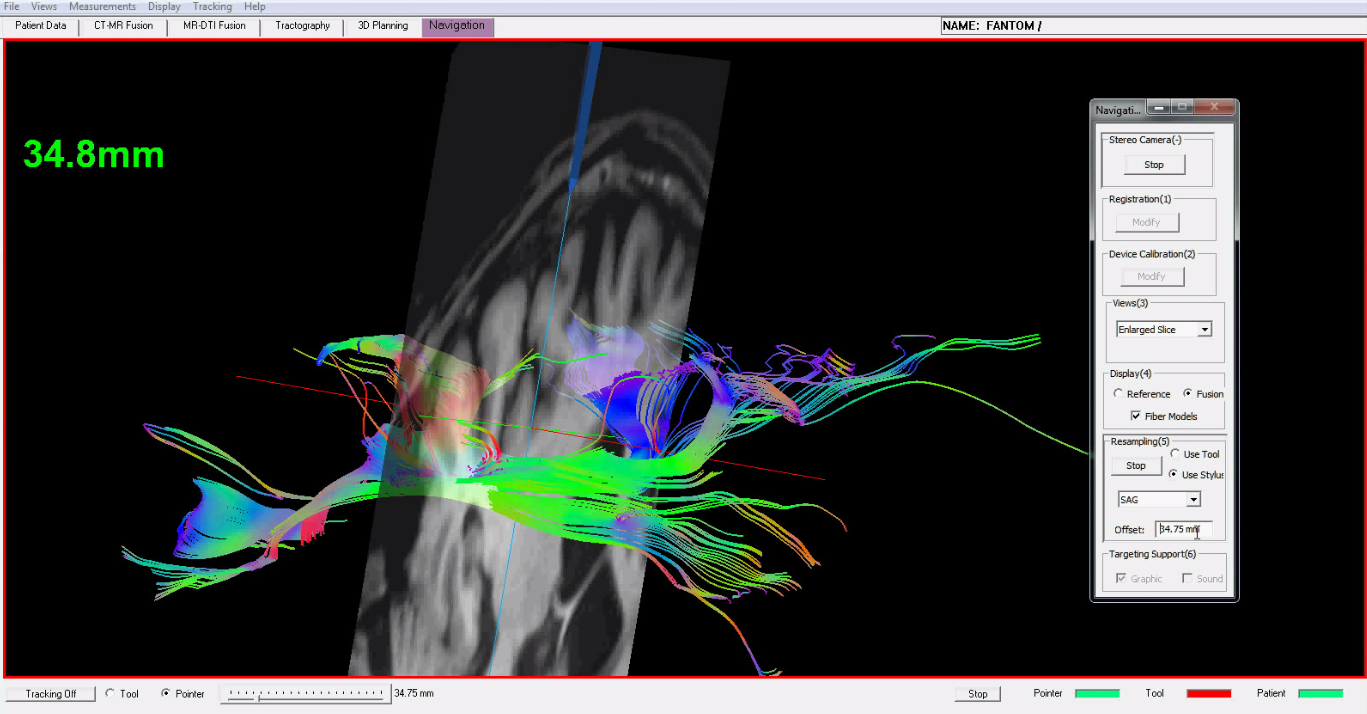
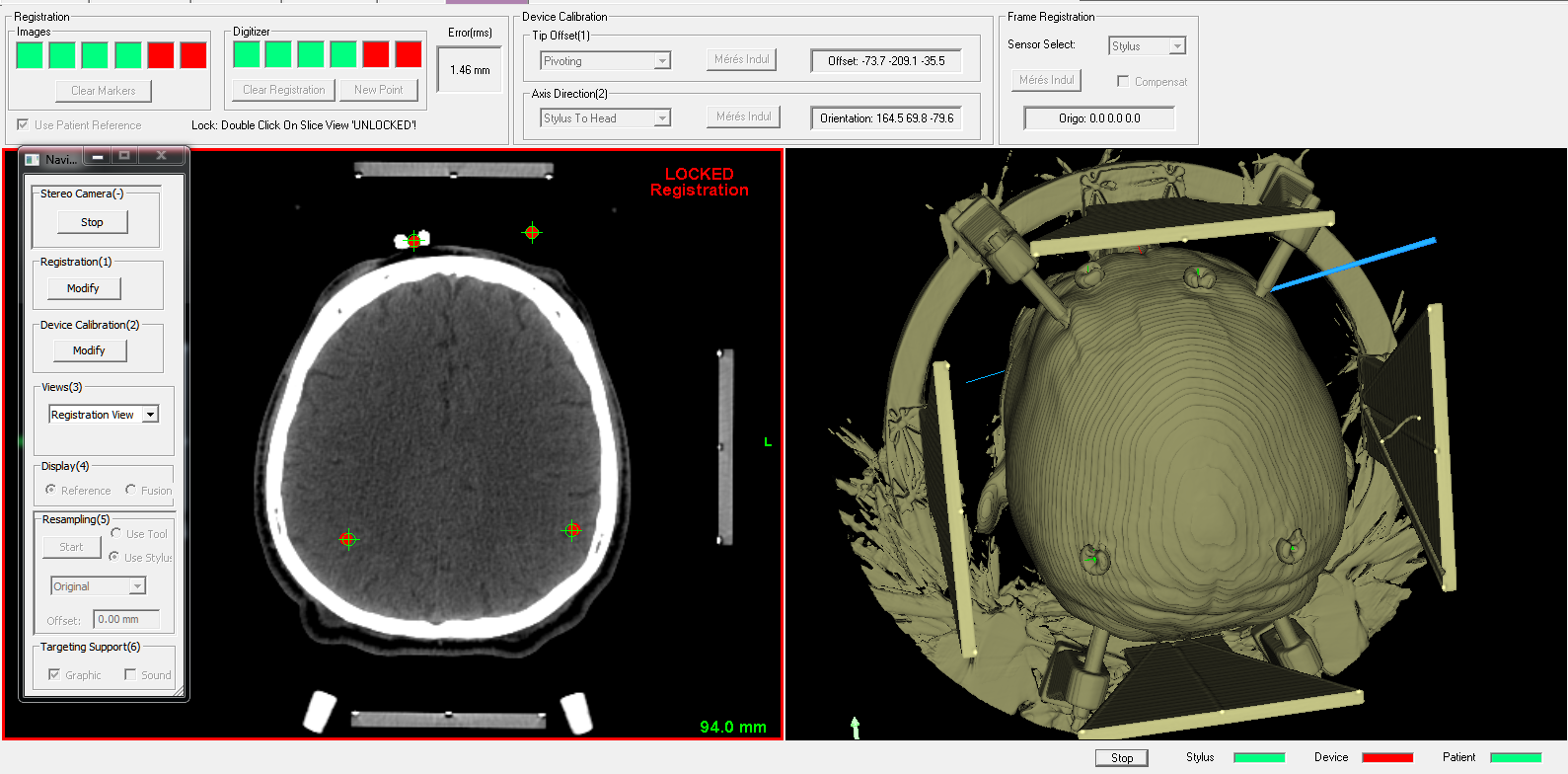
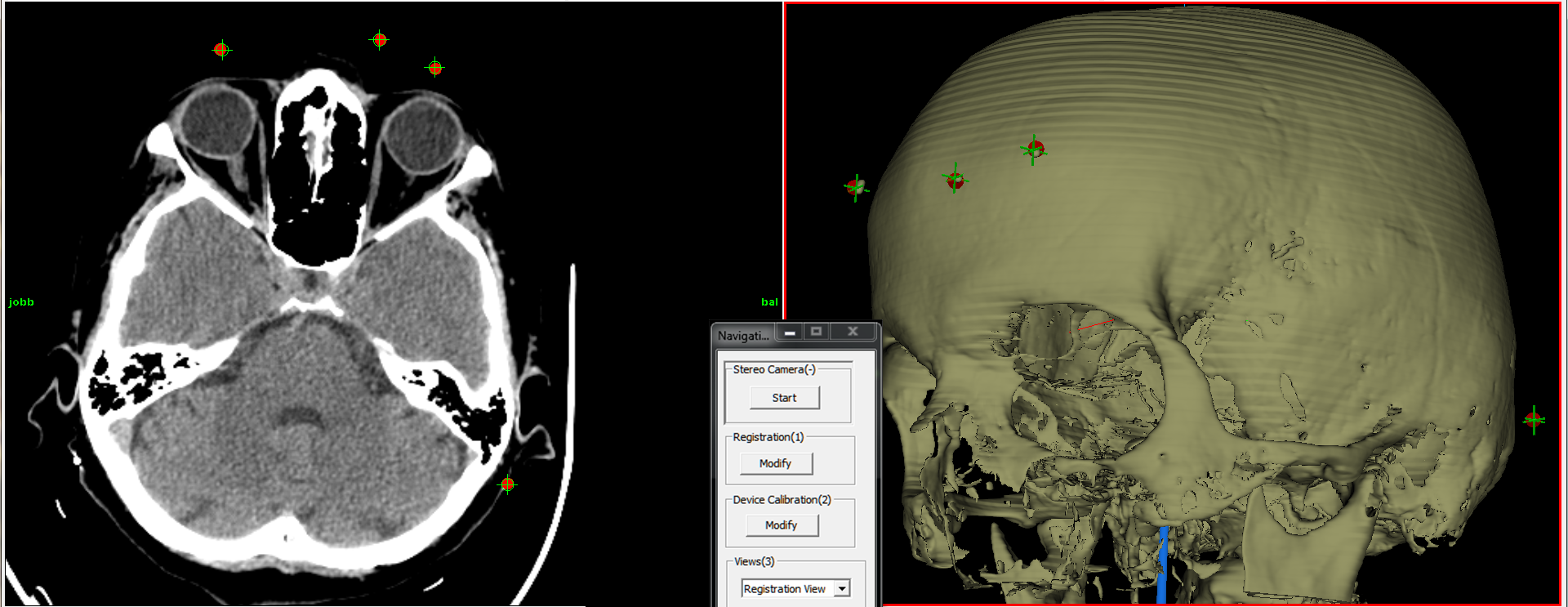
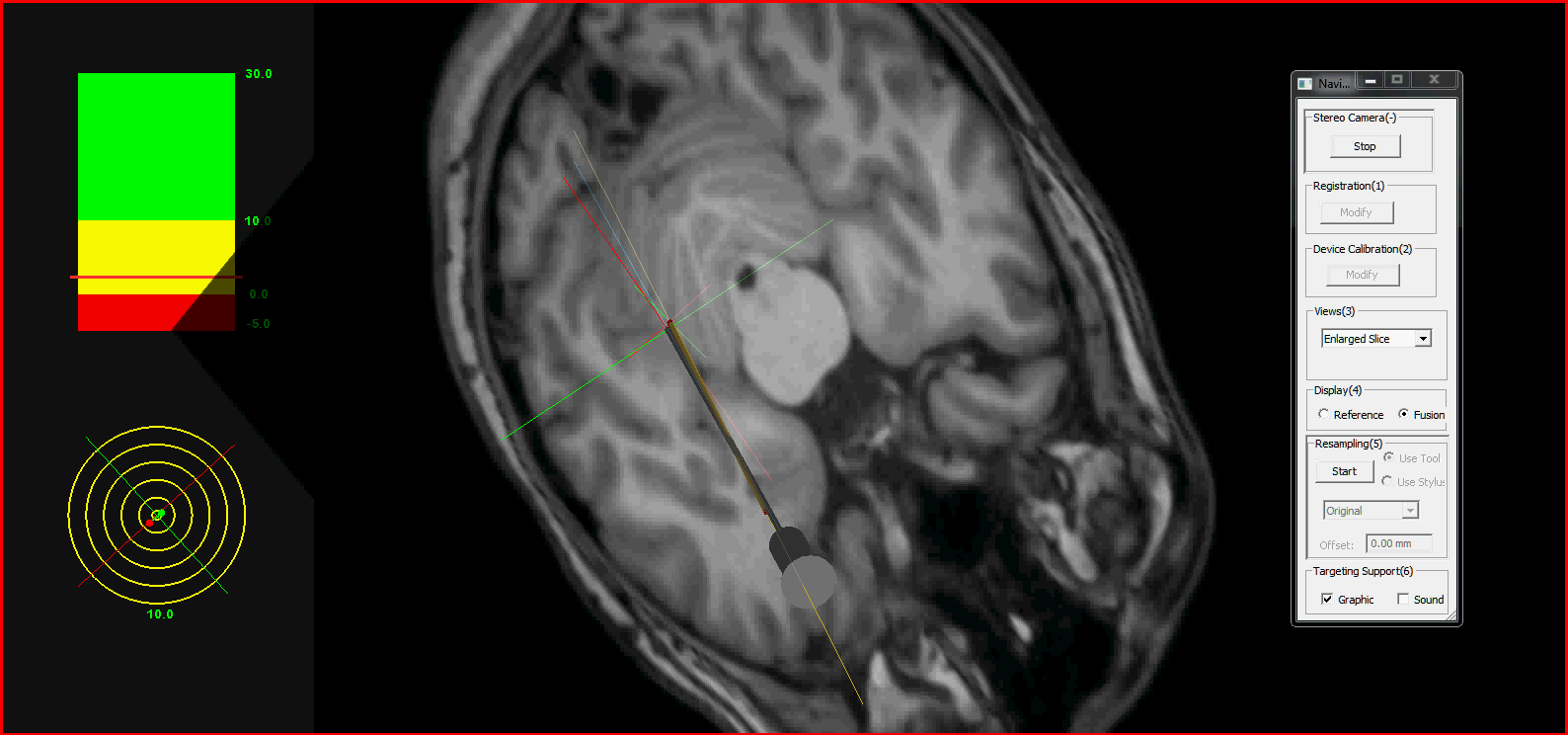
• Surgical Navigation module in frameless mode: planning results are usable in optical navigation after surgical space is registered by fiducials. Different tracking modes can be initiated for imaging data using real-time 3D resampling with optional display of fiber models.
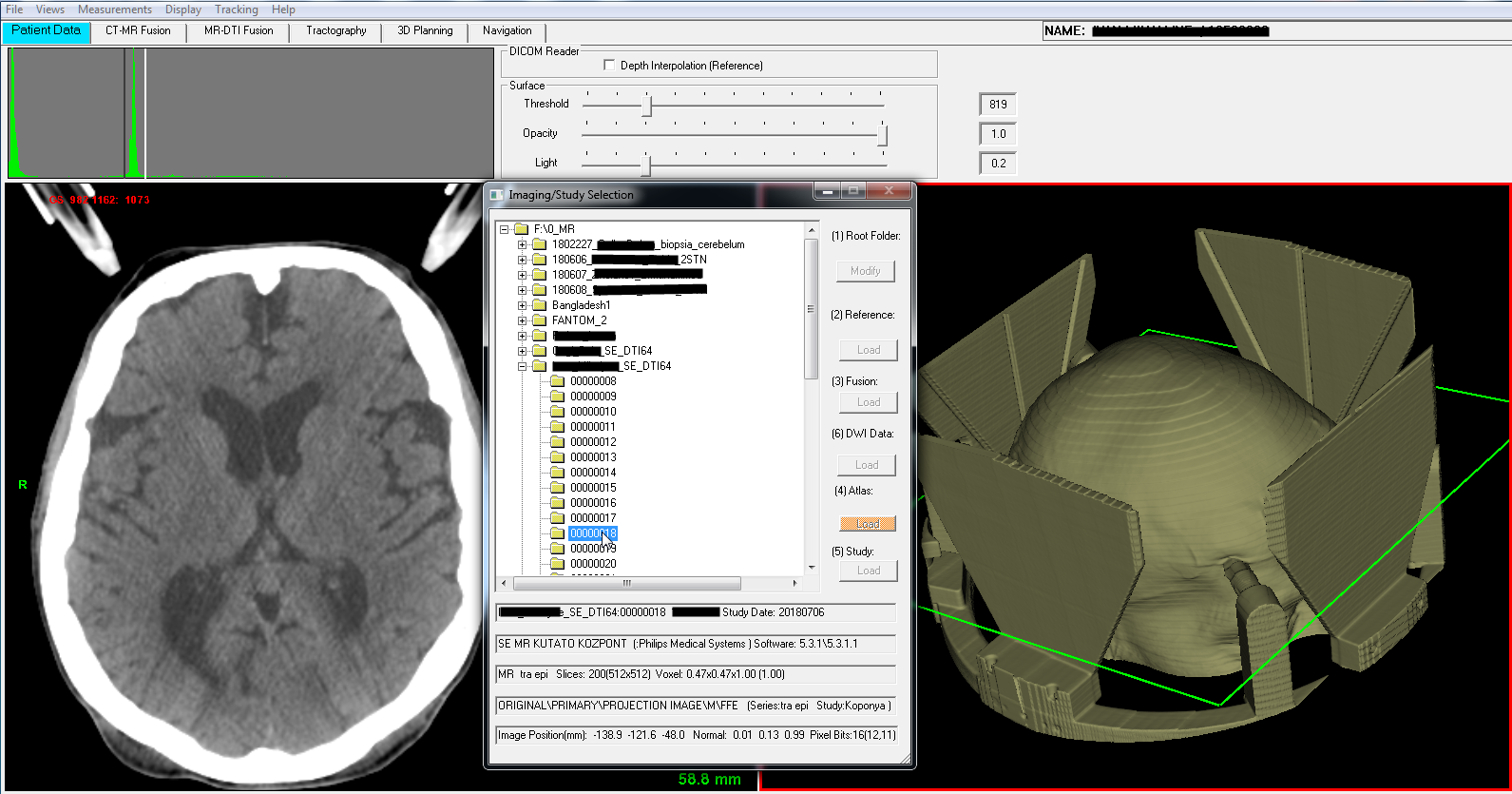
After automatic data parsing of diffusion data found in patient folder, the program generates unregistered DTI mask file and calculates/adds reference DTI volume from tensor images.
Fusion can be executed in next optional ways:
• using patient (or scanner) transforms extracted from DICOM headers (MR and DTI) and neglecting patient’s move during scanning;
• aligning 0 b-value map as reference to anatomical MR and executing motion compensation with CUDA-based algorithm for the full DTI data set;
• adding CUDA-based deformable registration between MR and reference DTI map to find forward and backward displacement fields;
• build up diagnostic imaging with fusioned ADC or FA maps as reference DTI.
Preferences for using DTI-MR data fusion in fiber modelling during stereotactic planning:
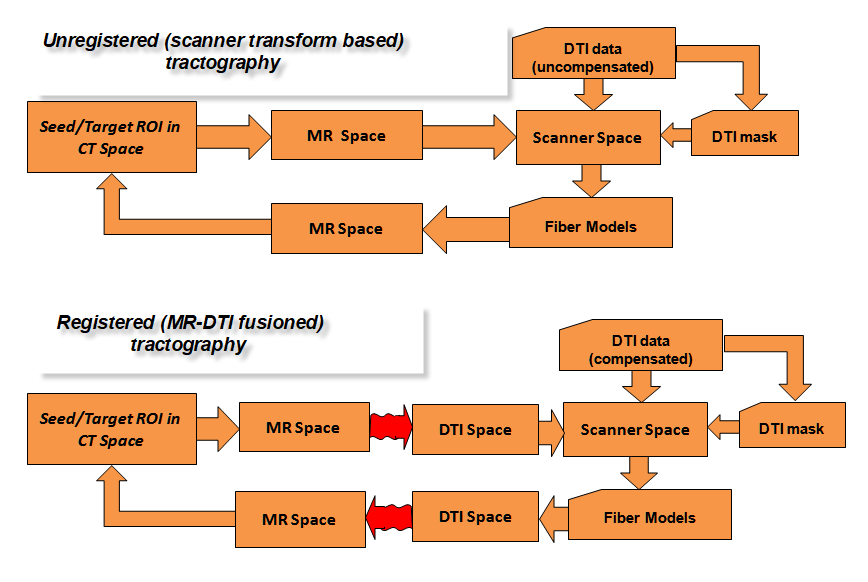
• Unregistered (scanner transform based)approach is very simple, only seed/target ROI mapping needed between the CT reference volume and original, raw MR volume. From there the scanner and DWI spaces can be reached where the uncompensated diffusion data with mask file is used for fiber modelling;
• 0 b-value map as DTI reference,after automatic rotation compensation with scanner transforms, it is aligned to anatomical MR by mouse. Motion compensation is executed with CUDA-based affine algorithm for the full DTI data set with registration to DTI reference. In this case the optimized DTI-MR projection transform is used to reach the diffusion space where the fiber models are calculated with compensated diffusion data and mask file;
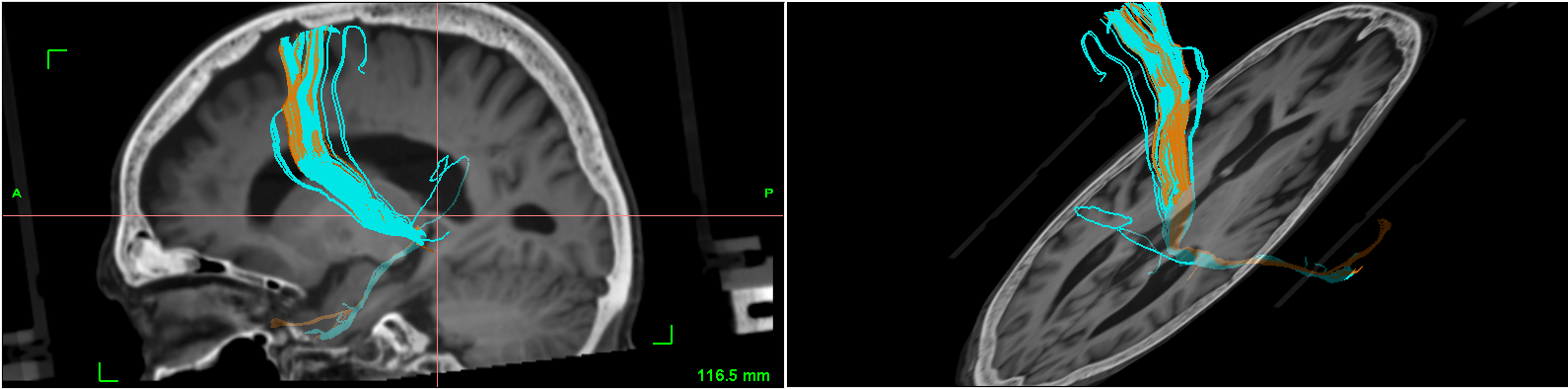
• CUDA-based deformable registrationis activated between MR and reference DTI map to find forward and backward displacement fields, followed by motion compensation as before. In this case the MR to DTI nonlinear displacement field is used to optimise seed/target ROI image data during tractography initialization. If tractography finished the resulted fiber models are mapped back from DTI to MR/CT volume using DTI to MR displacement field;
| Planning strategies in 3D | |
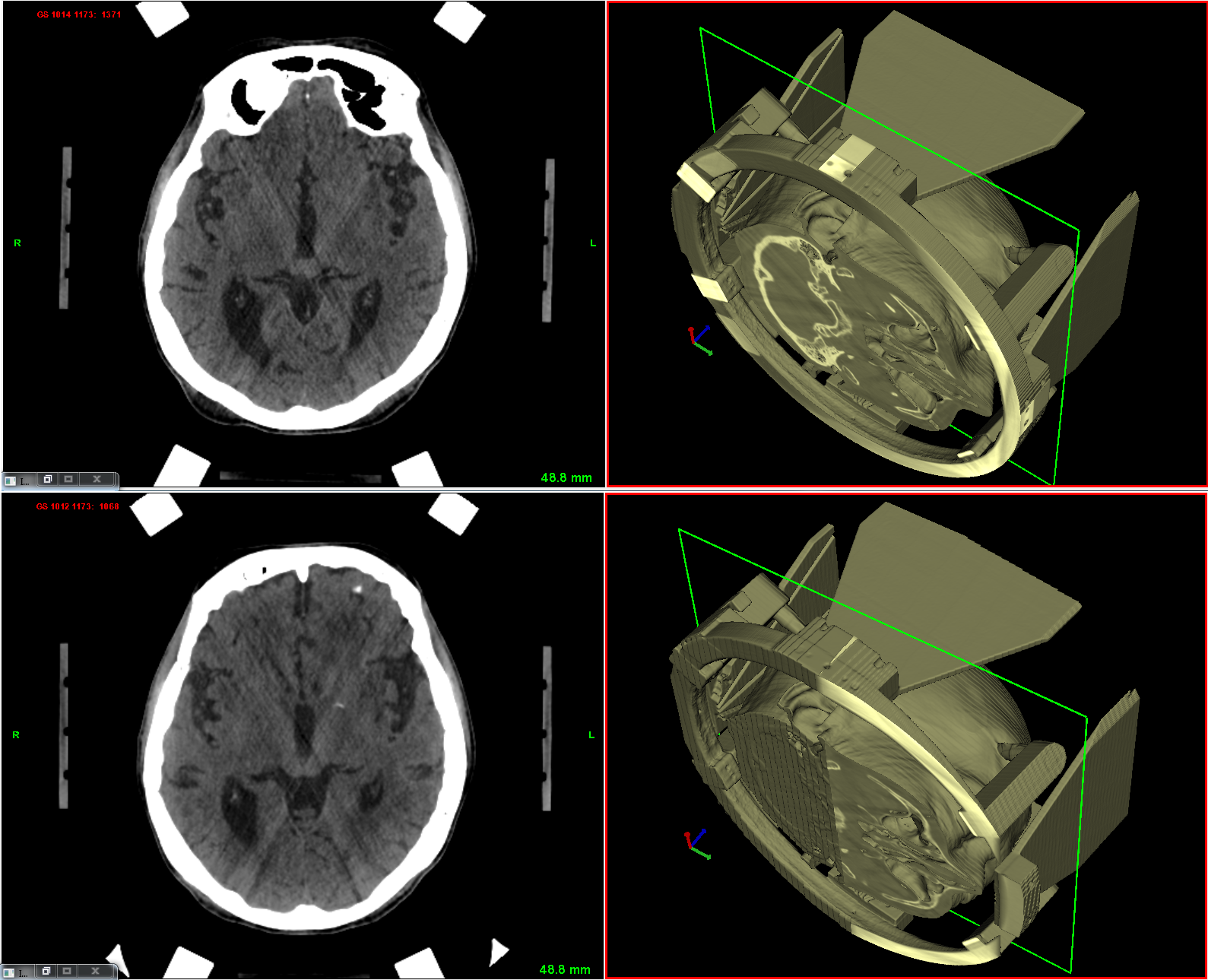
| Frame-based Interventions: | • 3D alignment planner to find the best representation of anatomy in imaging; |
| • Stereotaxy planner (Rotated mounting) by computation that helps to find generalized solution for different stereotactic frames. Continuous error feedback is added during marker localization; | |
| • Biopsy planner available in one side planner for biopsy; | |
| • Two sides trajectory planner according to anatomical symmetry for DBS (for some frames constrained optimization is selectable to keep left/right mounting on the same arc); | |
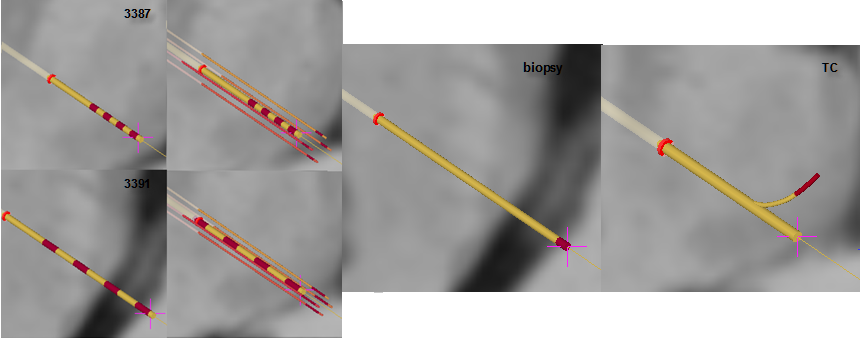
| • Wide selection of models of DBS electrodes (for stimulation and multiply recordings), biopsy needle and TC (thermolaesio) electrodes; | |
| • Export protocols of head-arc settings for operating room and study file storing full dataset of planning. | |
| Frameless Interventions: | • Orthographic trajectory planner using fusioned and different resampling views with optional data exchange with results of frame-based planning; |
| • Frameless mode:Surgical space registration using fiducials or anatomical markers (comparative accuracy test with frame-based method is possible); | |
| • Stylus supported calibration module Navigation of surgical device is possible if its simplified geometry is localized within the space of an attached motion sensor. This can be done with special calibration algorithm, Vister3D is able to simulate several navigated devices or add new surgical tools; | |
| • Communication softwarewith Polaris family of motion tracking cameras. Communication with motion tracking cameras from Northern Digital Inc. is configured by separate software which sets USB port connection. Back to modules |
Vister3D creates very flexible environment for surgical planning: the complex task of DTI registration to anatomic MR can be executed in preplanning step without using CT input. The results of this step are stored incompressed archive fileand can be inserted later into CT referenced stereotactic planning. Compressed archive studies can be generated and merged - with data integrity check - at different levels of calculation (after CT-MR fusion, stereotactic frame registration, trajectory planning, DTI fusion etc). Tractography can be performed not only during preplanning step but during on-site stereotactic planning, as well. The fiber models are exported to vtk file and can be imported later at any phase of planning. This improves the reliability of computations and creates a highly verifiable environment.
SurgiFront Ltd. has been owned by Ferenc Pongrácz, Dr. and his son Ádám Pongrácz. After working several years at Yale University (New Haven, USA) on the field of computational neurobiology Ferenc Pongrácz joined in pioneering work for implementing new motion tracking technology into medical applications. He worked for company Artma Biomedical Inc. (located in Salt Lake City, USA) which later moved into Vienna, Austria. He has many years of experience in developing software for various clinical fields listed from human motion analysis, integration of navigated endoscopic view into diagnostics, surgical planning and drill navigation in dentistry and recently stereoactic planning and navigation in neurosurgery. The application has been clinically pretested in routine surgeries with close supervision made by qualified surgeons. Vister3D has been also integrated into treatment of Parkinson's disease at medical care (DBS surgery and other minimally invasive procedures like radiofrequency ablation etc..). The software development has been supported by experts actively participating in open-source fields for medical applications. More info on related works: profile/Ferenc_Pongracz.
can be requested
from expert on computational method and surgical use of frame-based stereotaxy (Dr. István Valálik Ph.D. https://parkinson.hu/) and patients' database, workflow management, frameless navigation along with image fusion methods and tractography (Ferenc Pongrácz Dr. info@surgifront.com). Vister3D implements a flexible method for handling hierarchial topology of 3D surgical spaces (get info from Ferenc Pongrácz Dr. info@surgifront.com).
• Neuromed Private Care, Budapest, Hungary (https://neuromed.hu/)
SurgiFRONT Ltd.
Budapest, Zerind Vezér u. 29/B
1029 Hungary
phones: (+36) 305621806, (+36) 12758615
Contact email: info@surgifront.com